Indian Journal of Physiology
and Pharmacology
and Pharmacology
Indian Journal of Physiology and Pharmacology |
 (252x320).jpg) |
Volume 58 - Number 2 April - 2014 (Current issue) ISSN 0019-5499 |
Effect of skin to skin care to neonates on pulse rate, respiratory rate, SPO2 and blood pressure in mothersArchana Nimbalkar, Dipen Patel, Ankur Sethi and Somashekhar Nimbalkar |
Physiological benefits of skin to skin care (STS) to newborns are known but there is scarcity of data on changes in physiological parameters like pulse rate, respiratory rate, SPO2 and blood pressure in mothers during STS. We hypothesize that STS is beneficial to mothers with respect to these parameters. Objective of this study was to assess the changes of these parameters in mothers while providing STS for one hour. STS was provided by 52 mothers for a total of 127 times and parameters were recorded at starting of STS, at 15 min, at 30 min, at 60 min of STS and at 5 min rest after stopping STS. There were no significant changes in pulse rate and SPO2 but blood pressure and respiratory rate reduced significantly during STS as compared to rest after stopping STS. Thus STS is physiologically beneficial to mothers. |
Skin to skin care (STS) or Kangaroo mother care (KMC) began in Colombia in 1978 to help take care of neonates as an alternative to scarce and expensive incubators. Since then it is being increasingly implemented in the neonatal care units across the world (1). STS is provided to all the low birth weight infants (LWBI) during hospital stay and at home. Mothers are the primary caregivers to newborns. STS minimises separation between parents and newborns (2). Moreover STS improves breastfeeding, mother-infant attachment and infant growth (3). STS contribute to neurophysiologic organization, improves infant development, and also improves parental mood, perceptions, and interactive behaviour (4). STS is provided by keeping the newborn between
mother's breasts in prone position for at least one
hour to 24 hours a day. Multiple studies have
addressed the psychological impact of preterm birth
to mothers and have evaluated perceptions of
bonding/connection to her infant, post caesarean pain,
sensitivity to her infant's cues, anxiety and maternal
parenting confidence (5, 6). These studies do not
address the changes in physiology in terms of vital
parameters of the caregiver providing STS. Changes
in pulse rate (PR), respiratory rate (RR), SPO2 blood pressure (BP) in mothers during STS were
studied to confirm their stability during STS. We
hypothesize that there could be improvements in the
vital parameters of mother as psychological benefits
have been documented. |
A Prospective study of vital parameters of mothers providing STS to their LWBI was conducted in Neonatal Intensive Care Unit (NICU) of a medical college in Western India from April 2012 to February 2013. Rate of premature and LBW deliveries is approximately 20-25% and 40-45% respectively. All the staff nurses are formally educated in encouraging and guiding STS. The study population included the mothers of LBWI weighing more than 1000 g admitted to NICU were eligible to participate. STS was provided to physiologically stable newborns devoid of life threatening conditions and major congenital malformations. Mothers with fever or not able to provide STS due to other physical and mental conditions were not included. After consent, eligible mothers were taken through a brief comprehensive training session on practise of STS by trained nurses. Mothers were instructed to empty the bladder and wear the front open gowns with short sleeve to avoid the discomfort of tight fitting clothes. Due care was taken to minimize background noise. Mothers avoided eating at least an hour before starting STS. STS was provided in supine position for 60 min as per guidelines (7). Vital parameters including PR, BP, RR and SPO2 were recorded at the beginning of STS, at 15 min, at 30 min, and at 60 min of starting STS and after 5 min of rest after stopping STS from these mothers. In present study, vital parameters after rest of 5 min after stopping STS were taken as baseline parameters as 5 min rest is sufficient to get rid of effects of physical activity of stopping STS (8). Staff nurses were trained regarding the study procedure, and recording data in the study proforma. PR and SPO2were recorded using pulse oximeter of Philips (SureSigns VM6). RR was recorded clinically for 1 min. BP was recorded by using Omron automatic BP monitor with Intellisense Model [IA2 (HEM-7011-C1)] working on oscillometric principle validated with Diamond Conventional Mercury BP Model (Deluxe: BPMR 120). Validation of automatic BP monitor was done with each participant before the STS was started. Validation processes were based on guidelines of American Heart Association (8). Time interval was recorded by RACER stopwatch (Model SW 369). At each time, order of taking parameters was PR, SPO2 , RR and then BP. BP was taken at last to avoid effects of physical manipulation during taking BP. Enrolled mothers provided STS on once daily basis during any time of the day they were comfortable. From each mother, readings from minimum of 1 to maximum of 5 STS were taken. Statistical analysis Data from study proforma were transferred to SPSS
14 and mean of vital parameters were measured of
each time interval during STS and at rest. Analysis
was done using paired-t test to compare the changes
in vital parameters during STS to those at rest after
stopping STS. P value of less than 0.05 was
considered statistically significant. Study was
approved by Institutional Human Research Ethics
Committee. |
Total 75 mothers of LBWI were screened for STS. Of these 10 mothers were not eligible for STS as their newborns were physiologically unstable. Out of 65, 59 mothers gave informed consent for study. From these 59 mothers, recordings were incomplete in 5. The reasons were movement of 2 mothers leading to change in parameters; staff nurse had emergency work and were not available for data collection in 3 mothers. Two mothers were not comfortable in frequent BP recordings and opted out. Study procedures were completed in 52 mothers. Total 127 times one hour STS was provided by these 52 mothers. Age range of these mothers was 20 years to 40 years and mean age was 27.71(SD 5.20) years. Mean Body Mass Index (BMI) was 23.73+2.63 kg/ m2 . From these 52 mothers, 13 (25%) were overweight but none was obese as per WHO BMI standards. Mean and SD of PR, SPO2 , RR and BP readings at different time interval from 127 STS with significant difference as compared to rest after stopping STS are given in Table I. There were no significant changes in PR and SPO2 readings at all possible pairs (total 10) from beginning
of STS to at rest (P>0.05). At all time intervals, |
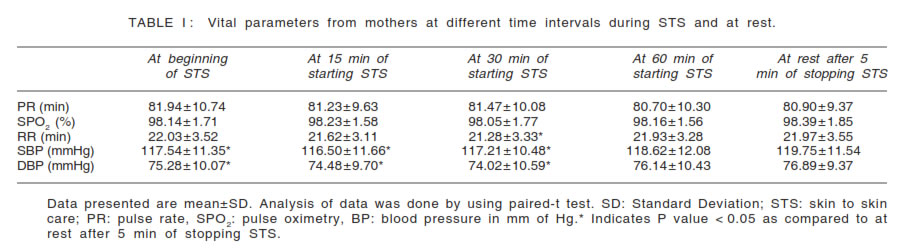 |
mean PR remained at 80 to 82/min and mean SPO2 remained at 98% to 99%. During STS there was significant reduction in RR at 30 min of STS as compared to those at beginning, at 60 min of STS and after 5 min of rest. Systolic and Diastolic BP readings were significantly
less at beginning, at 15 min and at 30 min of STS
as compared to rest. During STS, Systolic and
Diastolic BP readings at 15 min were significantly
less than at 60 min of STS. During STS, Diastolic
BP at 30 min was significantly less than at 60 min.
From these 52 mothers, 4 recorded elevated systolic
as well as diastolic BP; 1 had isolated elevated
systolic BP and 6 had isolated elevated diastolic
BP. All elevated BP readings recorded in this study
were in stage 1 category of hypertension as per the
guidelines published in special issue on Indian
guidelines on hypertension (I.G.H.) – III (9). All 5
mothers who had elevated systolic BP showed normal
readings during STS. Similarly from 10 mothers who
had elevated diastolic BP, 9 mothers recorded normal
readings during STS. |
During pregnancy due to changes in hormones and increasing physiological needs of growing fetus, the cardiovascular system of mother has to overwork. Pregnancy is a physiological process in which there is increased cardiac performance and progressive left ventricular remodelling (10). There is increased blood volume, cardiac output and maternal PR; decreased arterial BP and systemic vascular resistance in pregnancy and it takes weeks and months after delivery to get almost fully reversed (11). Physiological ventricular hypertrophy takes longer to resolve than the rest of the post-partum changes (12). Study done by Duvekot JJ noticed that these changes are greatest within 2 weeks postpartum (13). STS is implemented as early as possible in neonatal units when newborns become physiologically stable. This period is usually 5 to 7 days after birth in our unit in neonates weighing between 1000-1500 gm and 2 to 3 days after birth in neonates weighing between 1500-2000 gm. STS is immediately started after birth in physiologically stable LBWI more than 2000 gm. Thus STS is started usually within the first 2 post-partum weeks and these are the weeks of greatest changes in physiology after delivery. WHO estimates that 15 million newborns are born preterm every year and this number is rising (14). Increased incidence of prematurity would increase their numbers in NICUs and more mothers would experience separation from neonates. This would increase anxiety in mothers. During STS mothers report less stress, more positive feelings toward their infants and they feel their important role in parenting (15). Study on STS by MA Tallandini evaluated maternal emotional stress with the Parent Stress Index-Short Form questionnaire which showed significant reduction in maternal emotional stress (16). However these studies had not evaluated physiological changes in mothers during STS. Player MS and Peterson LE concluded that psychosocial stressor associated with anxiety raise the risk of hypertension and future development of coronary heart disease (17). We evaluated impact of STS on maternal vital parameters. The findings of reduction in systolic and diastolic BP as well as RR during STS as compared to rest could be because of stress relieving effects of STS to mothers, but we neither measured mental parameters in this study nor performed the blood investigations to find out the changes in hormonal physiology and hence we were not able to find out the reasons of changes in RR and BP during STS and at rest. Similarly we were not able to analyse the reasons for no change in PR and SPO . Logically STS should not reduce cardiac output and because of this, reduction in BP during STS without significant changes in PR suggests reduction in peripheral vascular resistance. Conclusion One hour STS improves maternal BP and RR and
has no impact on PR and SPO2
. STS has physiological benefits to mother. Considering at the
trends of drop in blood pressure during STS as
compared to rest following STS in mothers having
high readings, there is a scope for designing a study
on the effect of STS in mothers having high blood Limitations of the study Changes in vital parameters over days after delivery
were not studied. Study on mother's family risk
factors of hypertension, her dietary pattern and
physical activity were beyond the scope of this study.
We have not studied impact of STS on maternal
stress so correlation between maternal stress and
its relationship with vital parameters was not
evaluated. |
|